

When a patient suffers a cervical spine fracture, the right fractured neck brace directly affects healing outcomes, patient comfort, and even compliance. But with rigid collars, semi‑rigid supports, halo vests, and custom-molded options on the market, how do you choose the one that fits your clinical needs and inventory strategy? This guide breaks down the key types of fractured neck braces, their indications, and practical selection criteria—so you can stock smarter, support your healthcare clients better, and reduce return rates.
What Is a Fractured Neck Brace and Why the Right Type Matters?

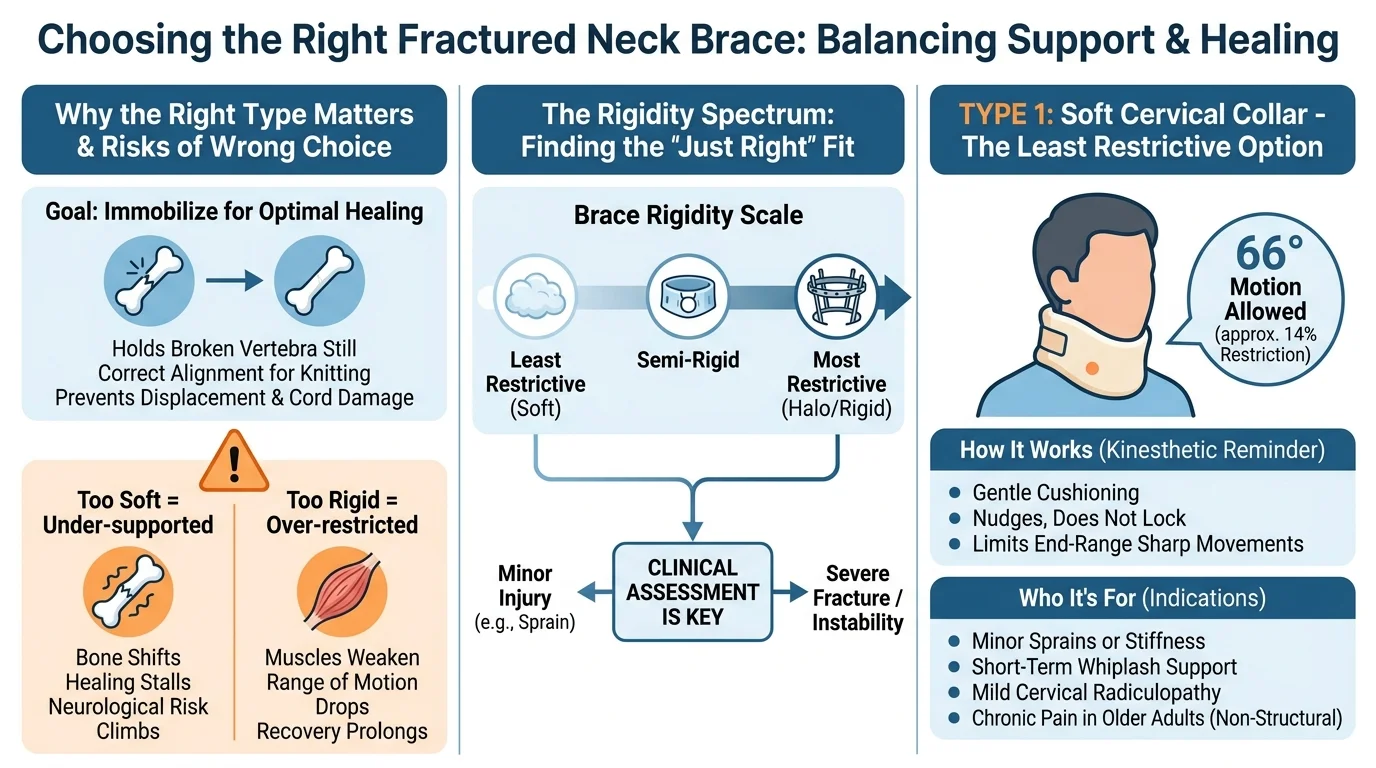
Bone doesn’t heal well when it moves. That’s the reason a fractured neck brace exists.
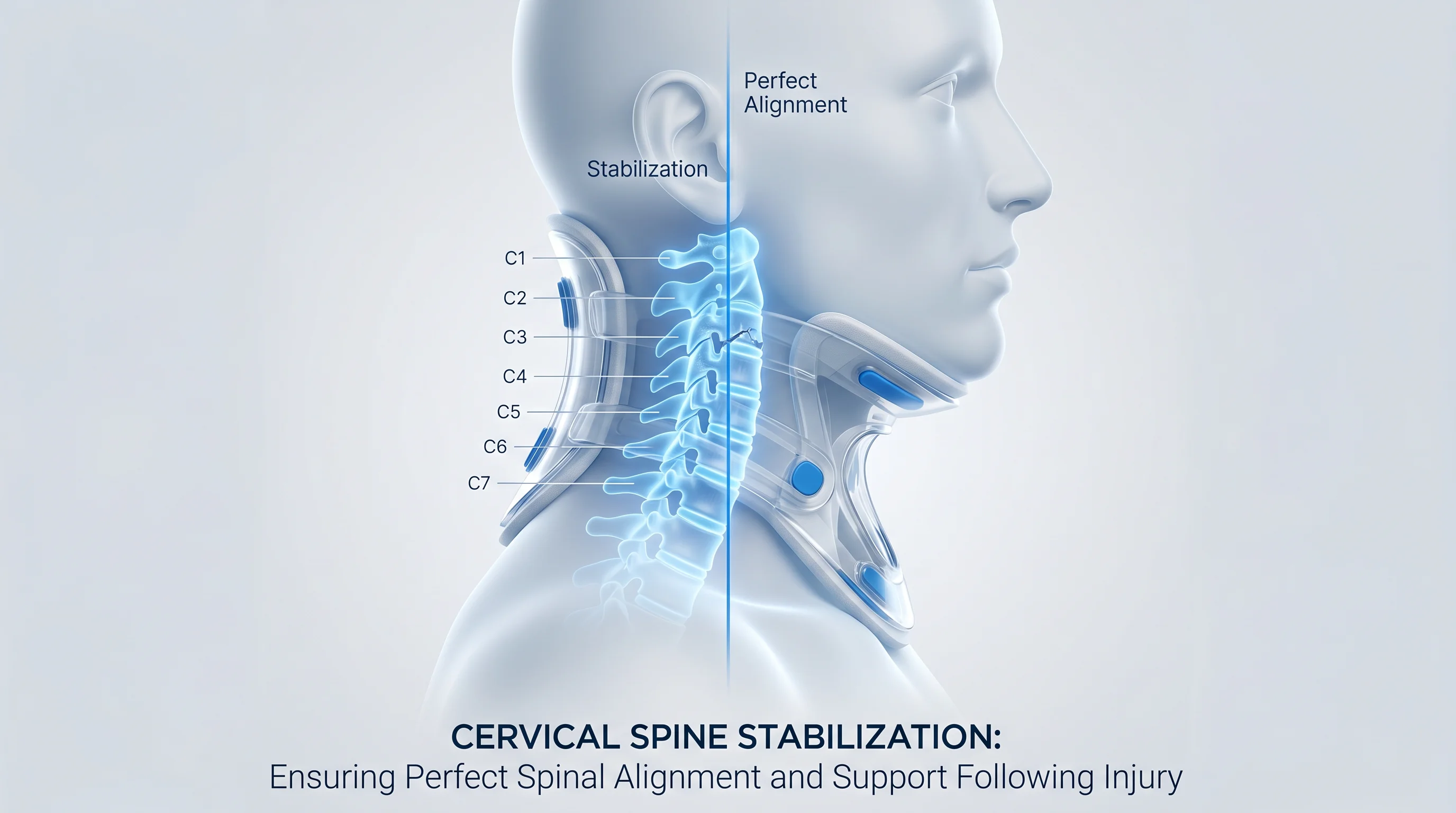
A cervical collar for a fracture does one thing above all else: it holds the broken vertebra still. It keeps the bone in correct alignment long enough for it to knit back together. Without that stillness, you risk displacement, failed healing, or direct damage to the spinal cord.
But most people don’t realize this at first. “Neck brace” isn’t a single thing. It’s a category. The devices inside that category vary widely. On one end, you have thick foam collars that offer gentle support. On the other hand, halo systems pin a metal ring to your skull and lock your head in place with rigid steel uprights.
Using the wrong type carries real consequences in both directions:
-
Too soft for your fracture — the bone shifts, healing stalls, neurological risk climbs
-
Too rigid for your injury — muscles weaken, range of motion drops, recovery takes longer than it should
Type 1: Soft Cervical Collar — Least Restrictive Option

A soft cervical collar is the most basic form of neck support you can get. A foam or felt core, wrapped in breathable fabric, secured at the back with a Velcro closure. No rigid plastic. No steel uprights. No pins. Just gentle, even compression around your neck.
How Much Motion Does It Restrict?
One comparative study measured soft foam collars allowing 66 degrees of cervical motion. That works out to 14% effective restriction of your total range of movement. You’re wearing a device that blocks about one-seventh of normal neck motion. The rest? Still available to you.
Soft collars work mainly as a kinesthetic reminder. They signal your body to move less sharply, limit end-range flexion and extension, and take the edge off nerve root irritation. They don’t lock anything down. They nudge.
Who This Fits
-
Minor cervical sprains or stiffness where structural stabilization isn’t required
-
Short-term whiplash support — though the evidence here is more precise than most people expect
-
Cervical radiculopathy with mild symptoms, where less motion reduces nerve irritation
-
Chronic neck pain in older adults as a short-term comfort aid
Precautions for Soft Cervical Collar Use
-
Clinical guidelines strictly limit soft collar wear to 7–10 days for acute whiplash or neck pain—WebMD explicitly advises against exceeding 10 days post‑injury. Beyond 10 days, the collar may hinder recovery by discouraging the muscle activity needed for cervical stability.
-
A less obvious risk: because soft collars feel mild, patients often wear them longer than indicated. Prolonged use accelerates muscle deconditioning, weakening the very muscles that support the spine. By the time the collar is removed, those muscles may be weaker than before.
-
There is also a psychological component: some perceived pain relief stems from the feeling of being supported, not from structural improvement. Therefore, subjective comfort should never be mistaken for a sign of healing.
Type 2: Rigid & Semi-Rigid Cervical Collar — The Most Common Fractured Neck Brace
Rigid and semi-rigid cervical collars are the go-to tool for fracture stabilization. Most people picture these when they say “fractured neck brace.” For stable, non-operative cervical fractures, they earn that reputation.
What Makes Them Different From Soft Cervical Collars
The construction makes the difference clear. Two pieces — front and back — built from thermoplastic foam with a rigid or semi-rigid plastic shell. Velcro straps pull the panels together. The full setup locks your head between the jaw and the sternal notch. It holds the injured area still and prevents movement.
That matters in a clinical setting. Rigid and semi-rigid designs restrict flexion, extension, and rotation far more than foam alone. That level of restriction lets fractures heal and ligaments repair — no surgery needed.
Fit Is the Whole Game
A collar that doesn’t reach the sternal notch won’t protect you. Chin support in the wrong position can cause the fracture to shift. In hospital settings, staff rechecks the fit every shift. Neck swelling changes how the collar sits. A loose collar on a fracture is a serious problem.
One Practical Note
Some semi-rigid collars handle shower use fine. Many rigid fracture collars don’t. Yours may need to come off for hygiene. Keep manual cervical immobilization in place the whole time. The collar coming off does not mean the fracture is stable.
For non-operative cervical fractures where a halo isn’t needed, this is your device. Get the right size. Make sure it fits well. Keep up with daily care. It does the job.
Type 3: Halo Vest (Halo Ring Brace) — Maximum Immobilization for Severe Fractures
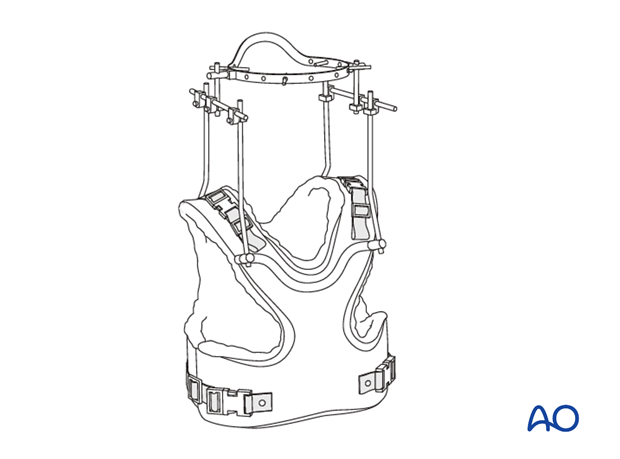
A metal ring bolted to your skull. Four steel pins torqued into bone. A rigid vest locked to your torso by upright rods. That’s the halo brace cervical system — and nothing external comes close to what it does for severe fractures. This is the top of non-surgical cervical immobilization. It connects your skull directly to your chest, cutting out almost all motion at the upper cervical spine.
Who It’s Built For
The halo brace targets the most serious upper cervical fractures — C1–C2 injuries in particular:
-
Jefferson (C1 burst) fractures
-
Type II odontoid fractures in younger patients
-
Type II and IIA Hangman’s fractures
-
Atlantoaxial injuries and C1–C2 dissociation
The Immobilization Isn’t Absolute
The halo vest does not fully immobilize the entire cervical spine. Subaxial motion can still occur between vertebral segments, even with the ring locked to the vest. The device cuts movement sharply at the upper cervical levels. It does not guarantee zero motion throughout.
That difference matters in practice. Locked facets, bilateral facet dislocations, and pure ligamentous injuries without fracture all tend to fail with halo treatment. The device was not built for those patterns.
Complications to Know
Pin loosening is the most common issue. Most cases resolve with retorquing or pin replacement. Infection, skin breakdown at pin sites, and pressure points are all manageable with consistent daily care.
The data on older patients carries a harder edge. Of the 5.6% who developed medical complications — cardiac or pulmonary — two out of three died within 30 days. The halo vest contributed to that decline. The vest limits chest expansion. That becomes a real problem for patients whose heart and lung reserve is already low.
Absolute contraindications rule out the halo ring brace entirely:
-
Complete spinal cord injury with anesthetic skin
-
Bone or disc fragments compromising the canal
-
Unreduced dislocation or subluxation
-
Progressive neurological deficit
For severe, unstable upper cervical fractures where surgery isn’t the path — the halo vest remains the strongest external option available. It earns that position. It also requires careful patient selection, exact fitting, and close follow-up at every stage.
Type 4: Cervicothoracic Orthosis (CTO) — Extended Control for Lower Cervical Fractures

Lower cervical fractures — C5, C6, C7 — sit in a mechanical blind spot. A rigid collar reaches there. It just doesn’t hold there well enough.
That’s the gap a cervicothoracic orthosis fills. The CTO extends below the collar line. It anchors to the thorax at T4–T6 using a sternal plate in front and a thoracic plate behind. Rigid uprights connect the cervical section to the thoracic anchor. The result: the rib cage does the holding, not just the neck.
Why the Extension Changes Everything
The numbers make it clear. A rigid collar — Miami J, Aspen — reduces flexion-extension at mid and lower cervical levels by 50–60%. A well-fitted CTO pushes that to more than 70–80% at the same levels. Lateral bending and rotation follow the same pattern. Collars manage around 50%. CTOs reach 60–70%.
For a C6 compression fracture or a C7 spinous process injury, that gap matters. It’s the difference between enough immobilization and falling short.
The cervicothoracic junction — C6 through T2 — is where collar control breaks down. At that level, fractures require thoracic extension to stabilize the junction.
Where It Sits in the Decision
-
Rigid collar — handles stable, lower-risk subaxial fractures
-
CTO — handles mid-to-lower cervical and cervicothoracic junction fractures that need more control than a collar can deliver
-
Halo vest — handles severe instability
Halo is sometimes off the table. Poor skull bone quality, infection risk, or patient age can rule it out. In those cases, a CTO becomes the strongest non-invasive option available.
Wear Protocol
Twelve weeks, 24 hours a day. That’s the standard. The device stays on in bed, during meals, through every part of the day. Most patients switch to a second set of inner pads each day. This helps manage moisture and reduces skin pressure at the occiput, mandible, sternum, and scapulae. Those are the areas where skin breakdown rates in prolonged rigid orthosis wear run between 10–30%.
Fractured Neck Brace Comparison: Side-by-Side at a Glance
Here’s what the research shows — motion allowed as a percentage of normal cervical range:
|
Brace Type |
Flexion/Extension |
Lateral Bending |
Rotation |
|---|---|---|---|
|
Halo vest |
4–12% |
4–8% |
1–2% |
|
Yale CTO |
12.8% |
50.5% |
18.2% |
|
Minerva jacket |
14.0% |
15.5% |
0% |
|
Four-poster brace |
20.6% |
45.9% |
27.1% |
|
SOMI brace |
27.7% |
65.6% |
33.6% |
|
Philadelphia collar |
28.9% |
66.4% |
43.7% |
|
Soft collar |
74.2% |
92.3% |
82.6% |
A lower percentage means more restriction. More restrictions mean more healing protection.
Three things stand out from that table:
-
Rotation is the hardest plane to control. The Minerva achieves a full rotational block. Every other brace allows some rotation.
-
The halo leads to upper cervical immobilization. The Minerva matches or beats it on lateral bending and rotation at lower levels.
-
The soft collar does little as a stabilization device. It keeps over 70% of motion in every plane. That’s too much freedom for a serious fracture.
How to Choose the Right Fractured Neck Brace: Key Decision Factors
1. Fracture pattern and stability come first.
Your imaging provides information: CT, X-ray, and MRI together. Unstable fractures and post-surgical fusions need rigid immobilization.
2. Match the fracture level to the device.
Upper cervical injuries (C1–C2) need maximum restriction — often a halo or high-profile CTO. Lower cervical fractures (C5–C7) need a CTO, not just a collar. A standalone collar loses mechanical leverage below C5, so a collar alone won’t do the job.
3. Fit is clinical.
Start with the front panel under the chin — that’s the single most important fit factor. From there, check these three things:
-
1 finger breadth between the collar and the neck during normal wear
-
2 finger breadths during meals to allow jaw movement
-
Straps of equal length on both sides; the chin centered on the rest
A collar that fails the finger test isn’t adjusted — it’s the wrong size. Don’t force the fit.
4. Skin risk changes the equipment list.
Older patients, diabetics, and anyone with fragile skin need thicker removable pads, smoother edges, and straightforward pad replacement each day. Skin breakdown rates in long-term rigid orthosis wear run 10–30%. That’s not a small number, so plan for it from day one.
5. Wear duration shapes the whole plan.
Fracture healing requires 4 to 24 weeks of full-time wear. Build the weaning schedule in from the start. Once healing allows, remove the brace for one hour in the morning and one hour in the evening. Add 30–60 minutes of brace-free time per session each day. Complete the full wean over one to two weeks.
6. Routine activities need a clear protocol.
Driving in a hard collar isn’t safe. Switch to a soft collar for the trip, then put the rigid collar back on arrival. Sleeping in a rigid collar is standard for the first two to three weeks. After that, many surgeons allow a soft collar at night — as long as morning pain stays under control.
7. Choose the least restrictive device that still meets the fracture’s stability needs.
Long-term rigid immobilization brings real complications: muscle weakness, swallowing problems, and pressure injuries. The goal is solid protection, not maximum hardware.
Wearing Guide: Getting the Most From Your Cervical Fracture Brace
How Long and How Often
Full-time means full-time. Most cervical fracture braces are prescribed for 24 hours a day. The one exception is hygiene, and only if your surgeon allows it. Remove the collar for the shortest possible time — under 10–15 minutes per session.
You wear it until healing is confirmed. That’s 6–12 weeks for most people, but your surgeon sets the timeline based on imaging.
Putting It On: Do It Lying Down
Put on a cervical fracture brace flat on your back, no pillow, head still, and facing the ceiling.
-
Slide the back shell first — push it into the mattress and guide it under your neck without lifting your head
-
Scoop the front shell up under the chin, tuck its edges inside the back piece, and fasten the Velcro straps in even tension on both sides
Then run the fit check:
-
Text on the collar reads right-side up
-
You cannot slide your chin in and out — if you can, it’s too loose
-
No plastic touches skin anywhere — pads sit between plastic and neck at every contact point
-
The collar doesn’t dig into the shoulder blades or rest on the collarbones
Taking It Off: Never Alone
Always have a helper for removal. Lie flat, no pillow, head held still. Your helper undoes one strap first. Then the front shell comes off while the back shell stays in place. Next, clean and dry the skin, check for redness, replace the front pads, and refasten. Then move to the back shell.
Any redness lasting more than 20–30 minutes after removal is a signal. It means the fit needs adjustment.
Call Your Care Team Right Away If You Notice
-
New or worsening numbness, tingling, or weakness in your arms or legs
-
New balance problems or difficulty walking
-
Severe pain that ice and medication don’t touch
-
Any open sore, blister, or redness that doesn’t fade after a pad change
Conclusion
Choosing the right fractured neck brace is about patient outcomes, comfort, and long-term recovery. Whether you need rigid cervical collars for stabilization or softer options for early-stage management, the key is working with a partner who understands both the science and the supply chain.
At AOFIT, we engineer solutions. As a CE/FDA-certified medical brace factory with ISO 13485 compliance, we serve over 160 countries. From spinal supports to post-op rehabilitation series, our product line covers every medical scenario, and we’re ready to customize according to your specifications.
Looking for a reliable partner for your orthopedic brace sourcing? Visit our medical brace factory page to explore our capabilities, certifications, and customization options. Let’s talk about how we can support your next project.